50 yrs old with HFrEF with DCMP secondary to ischemic heart disease
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Team:
Interns-
M Supriya
Mohitha
K Sowmya
Sanjay
Amrutha
Dr.Druga Krishna PGY1
Dr.Ajith Kumar PGY2
Dr.Laxma Reddy PGY3
Dr.Manasa PGY3
Dr.Vijaya Lakshmi (Ast.Prof.)
50 years old male presented on 4/3/21 to GM OPD with
C/o pedal edema from 10 days
C/o SOB from 10 days
C/o decreased urine output from 10 days
C/o abdominal distension from 10 days
Patient was apparently asymptomatic 10 days back then he developed pedal edema which is extending upto knee,acute in onset, gradually progressive, pitting type, no aggravating and relieving factors.
He has shortness of breath from 10 days, Grade 2 progressed to grade 3.
PND +
He has abdominal distension from 10 days.
No h/o chest pain, palpitations, sweating, syncopal attacks.
He has decreased urine output from 10 days.
No burning micturition or hematuria.
H/o injury to the Right foot over little finger 4 month back ,wound is been increaseing in size due to itching
Past History
K/c/o DM from 3 yrs (on irregular medication)
K/c/o HTN from 2 months and on Tab TELMA 40/12.5mg
No h/o epilepsy, TB, asthma, thyroid disorders.
-Personal History-
Intake of alcohol occasionally.
Smoking 5 packs/day.
O/E
Patient c/c/c
pedal edema + from 10 days
No H/o pallor, icterus, cynosis, clubbing,koilonychia, lymphedenopathy



Vitals-
BP-160/100 mmhg
PR- 84 bpm
RR- 22 cpm
Weight- 62kgs
-Systemic Examination-
CVS-
---inspection---
JVP-not elevated
No parasternal heave
apical impulse -no visible
no engorged veins,
---palpitations---
apex beat felt at 0.5cm lateral to the mid clavicular line in 6th intercostal space
All inspectory findings confirmed
---percussion---
Hearts boarders percussed
---Auscultation---
s1,s2 +
no murmurs
RS- BLAE+
NVBS+
P/A- soft, non tender
CNS- NAD
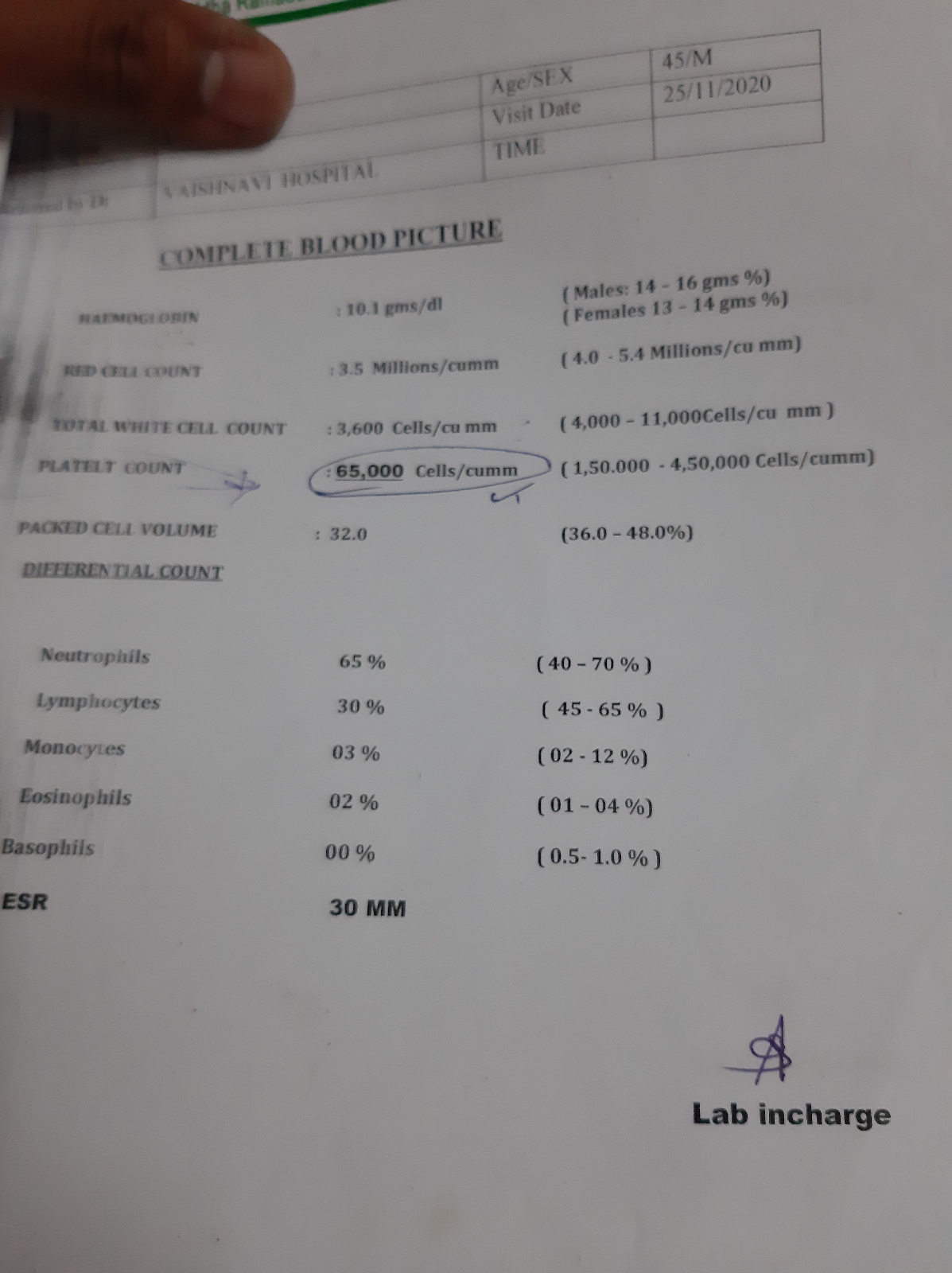
Investigations
2D ECHO-
EF- 30%
All chambers dilated
Global hypokinesia
Severe LV dysfunction
Diastolic dysfunction +







Treatment
1.Tab LASIX 40MG PO/OD
2.TAB ATORVASTATIN 40MG PO/BD
3.INJ NPH INSULIN/ SC
8U............x...........8U
4.INJ HAI / SC
8U..............8U........8U
5.INJ MONOCEF 1GM/IV/BD
6.TAB PENTOXFILLINE 400MG PO/BD
7.TAB RAMIPRIL 2.5MG PO/OD
8.TAB ULTRACET 1/2 TAB PO/QID
Provisional diagnosis-
HFrEF with DCMP secondary to ischemic heart disease with hypertension with type 2 diabetes mellitus.